pelvic pain

Women that live with pelvic pain on a daily basis deserve the best help and support available from a multi- disciplinary team of health professionals. For many women this is a really difficult subject to talk to their GP about. They may not go to see their doctor for fear that he or she may need to do an internal examination and this thought alone is terrifying for some women and puts them off…possibly for years! It is the GP’s job to help find the ’cause’ of your pain and refer you for appropriate tests or consultation to other health professionals/specialists.
Currently Dyspareunia and Vaginismus still fall into the Diagnostic and Statistical Manual of Mental Health Disorders. So the first referral is often to a sex therapist or psychologist. This may be necessary if there is significant emotional concerns for the patient. Many Pelvic conditions have ‘Musculoskeletal’ (muscle,ligament and joint) involvement. With careful, appropriate pelvic floor physiotherapy some women with pelvic pain can be helped tremendously. Pelvic floor physiotherapy is NOT just about strengthening the muscles!! Watch this video Amy Stein has published books on the treatment of pelvic floor pain. (check out Amazon – heal pelvic pain)
‘Pelvic pain’ is a general term for pain in or around the pelvic area. It encompasses bone, muscle, fascia, organs, and vessels including blood vessels, nerves and nerve sheaths. CHRONIC PELVIC PAIN is generally described as pain in your pelvic region — the area below your belly button and between your hips — that lasts three months or longer. There are many, many sub-divisions of this topic and I have touched on some of them under the ‘pelvic floor’ page. My focus on this page will be the treatment for clients with chronic pelvic pain CPP.
There is also a substantial amount of information about understanding how Chronic Pain is constantly driven by connections from our spinal cord to our brain and then an’up- sensitising’ of pain in the brain…..The brain decides whether you are going to have pain or not! This website “The pain toolkit” is a great resource to understanding how to start helping yourself
Dyspareunia
Dyspareunia is pain at the entrance to; and/or inside the vagina, just before, during or after sexual intercourse. The vagina is a muscular tube providing a passage between your uterus and the outside of the body. It has three functions: admitting the penis during sexual intercourse, allowing menstrual blood to leave the body, and giving birth. The labia minora are folds of hairless skin containing sweat glands that make up part of your external genitalia. The clitoris is a pea-size sexual organ located in front of the urethra, close to where the labia minora meet. It is highly sensitive with over 8,000 nerve endings and functions for sexual pleasure.
The location and frequency of pain with dyspareunia may vary. Symptoms often include: Pain at the entrance of the vagina with initial penetration; even from penetration from a finger or tampon Deeper vaginal pain with movement of the penis Pain may be a sharp and burning, or deep and aching You may also experience an involuntary tightening of the pelvic floor muscles (vaginismus) during penetration. The tightening can be severe enough that the vagina is unable to be penetrated.
There are several causes of dyspareunia, these include:
Vaginal dryness
Inadequate lubrication can be due to a lack of sexual arousal, or a decrease in estrogen, which occurs after menopause, during and after pregnancy, and while breast feeding.
Side effects of medications
Certain medications can decrease sexual arousal and result in inadequate lubrication. These medications include antihistamines, antidepressants, birth control pills, breast cancer medication, high blood pressure medication, and some sedatives.
Infection
A bacterial or fungal infection of the vagina, genital area or urinary tract can cause pain.
Inflammation or skin problems Inflammation or severely dry skin such as eczema can lead to painful initial penetration. Skin diseases such as lichen sclerosis or lichen planus can affect the vaginal area and lead to pain. Check out this video for more info on painful sex after pregnancy
Vulvar vestibulitis
A condition that can result in severe pain and sensitization on the area of the vestibule when touched or with initial penetration. Vulvar diorders include ; Lichen Planus
International Society for Study of Vulvar Disease www.issvd.org National Vulvodynia Association www.nva.org
Allergic reaction
An allergic reaction to clothing, spermicides or douches can cause painful intercourse. It can be seen on the vuval area and or inside the vagina on the mucosal lining. referral to a dermatologist specialising in Vulvo-vaginal conditions is the ideal pathway. caredownthere is another website offering excellent information and education.
STIs
Sexually transmitted infections s can cause blisters and sores that make intercourse painful. Uterine and other pelvic conditions
Certain conditions of the uterus can lead to painful intercourse. These conditions include retroverted uterus, endometriosis, pelvic inflammatory disease, fibroids, ovarian cysts, and interstitial cystitis.
Prolapses
A prolapse of the bladder (cystocele), uterus (uterine prolapse), rectum (rectocele), or intestine (enterocele) can cause a deep pain during intercourse.
Scarring
Previous surgeries to the pelvic area can cause scarring that may lead to painful intercourse.
Childbirth tearing of deep pelvic floor muscles or fascia; or an episiotomy during vaginal delivery may lead to painful intercourse. It is wise to delay sex until after your 6 week check up and then only when you and your partner feel ready. I encourage my mums to talk about how they feel to me and to their partner. Often the partner is very anxious about penetration and causing ‘any pain’. take things slow, use lubrication (I like Sylk) and try being on top for this first time so that you can control the depth of penetration. Some women are not ready to have sex for a long while after a difficult vaginal delivery.
Come and see your Women’s health physio so that she can examine you and then discuss your concerns.
Treatments for cancer Chemotherapy and radiation to the pelvic area can lead to painful intercourse.
Other traumas from sport or road traffic accidents and injuries to the pelvic area can cause changes to joints and muscles around the hips and pelvis. Over time this may cause chronic muscle tensions ligament, tendon and fascial tightness in and around the pelvis. This can lead to painful intercourse. Women’s health Physios treat muscles,joints and tendons.
Emotional factors can also contribute to painful intercourse. Emotions and stress are important for sexual arousal and greatly affect the amount of lubrication and the tightness of the pelvic floor. Psychological issues such as anxiety, depression, and fear of intimacy can be a factor with dyspareunia. Additionally, any history of sexual abuse can lead to problems with dyspareunia. Women’s health physios with a special interest in treatment of this condition can, as part of a multi -disciplinary team do a great deal to help with musculoskeletal changes that impact on pain and function.
Vaginismus
An involuntary tightening of your superficial pelvic floor muscles during initial penetration.Primary vaginismus is a spasm or dysfunction of the superficial pelvic floor muscles that can be helped with specific pelvic floor physiotherapy. Specific skills in the treatment of internal and external trigger points in muscle and releasing techniques directed to fascial and scar tissue help in the rehabilitation of this condition. Education of pelvic anatomy and an understanding of the ‘central sensitization of pain’ will all help individual women to overcome CPP.
Endometriosis
Here are some excellent websites that will help fill in your information gaps for this difficult condition. This first website has a really good education content on understanding this condition and how it may affect you now and in the future.
The Centre for Advanced Reproductive Endosurgery http://www.sydneycare.com.au/care-endometriosis-check-lis
Also the Jean Hailes Website (see website listing on right hand side of this website) This is a wealth of really factual information. There are many fact sheets to help you understand different problems.This is the Endometriosis fact sheet.
The following are a list of websites that may help;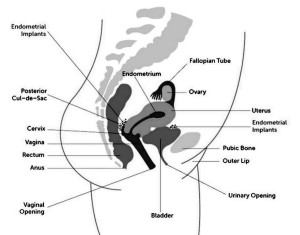
- http://www.equilibriahealth.com.au/Page/pelvic-pain-endometriosis
- http://www.equilibriahealth.com.au/index.cfm
- http://youngwomenshealth.org/2013/05/23/endometriosis-info-for-friends/
IBS -irritable Bowel Syndrome
“IBS is a group of symptoms that occur together, not a disease. In the past, IBS was called colitis, mucous colitis, spastic colon, nervous colon, and spastic bowel. The name was changed to reflect the understanding that the disorder has both physical and mental causes.
IBS is diagnosed when a person has had abdominal pain or discomfort at least three times a month for the last 3 months without other disease or injury that could explain the pain. The pain or discomfort of IBS may occur with a change in stool frequency or consistency or be relieved by a bowel movement.
IBS is often classified into four subtypes based on a person’s usual stool consistency. These subtypes are important because they affect the types of treatment that are most likely to improve the person’s symptoms. The four subtypes of IBS are
•IBS with constipation (IBS-C) ◦hard or lumpy stools at least 25 percent of the time
◦loose or watery stools less than 25 percent of the time
•IBS with diarrhea (IBS-D) ◦loose or watery stools at least 25 percent of the time
◦hard or lumpy stools less than 25 percent of the time
•Mixed IBS (IBS-M) ◦hard or lumpy stools at least 25 percent of the time
◦loose or watery stools at least 25 percent of the time
•Unsubtyped IBS (IBS-U) ◦hard or lumpy stools less than 25 percent of the time
◦loose or watery stools less than 25 percent of the time”
Physiotherapists don’t treat a lot of these conditions that I have listed, but the effect of these problems may cause associated muscle tensions within the pelvic floor. Sometimes the condition can be mild and only cause occasional pain,slowly becoming more of a problem as you try and become sexually active.Women’s health Physiotherapists trained in the treatment of pelvic pain can help to reduce the muscle tensions, address the pain and work with your doctors to establish the underlying cause. We can offer advice and refer on to appropriate health practitioner.
Pudendal Neuralgia
Pudendal Neuralgia can affect men and women. It is defined as burning, stabbing, and/or throbbing pain in the distribution of the pudendal nerve. The pain typically increases with sitting and exercise, and decreases with standing and rest. The pudendal nerve supplies most of the skin,labia and superficial pelvic floor muscles. Pain can be felt around or inside the vagina. Patients with pudendal neuralgia commonly have pelvic floor dysfunction as well as pain. Patients may report urinary dysfunction such as dysuria, (difficulty or pain on urination) urinary hesitancy, urgency, and frequency, and/or bowel problems such as constipation and difficulty evacuating. Some patients may also experience sexual dysfunction such as dyspareunia,(pain on penetration of the vagina) aorgasmia,(inability to reach orgasm) and post-ejaculatory pain. Common causes of pudendal neuralgia include chronic constipation, chronic urological or gynecological infections, and repetitive sporting activities such as bicycling and strong abdominal and ‘core’ type exercises.
This info sheet from WHIRA on Pudendal neuralgia gives you more understanding of the examination and treatments available for this condition.
The Society for Pudendal Neuralgia (SPuN)
Women’s Health & Research Institute
Prof Thierry Vancaillie, Gynaecology & pain medicine (public & private practice, referral required) Vulvodynia / pudendal neuralgia, pelvic & perineal pain
Level 12, 97-99 Bathurst St, Sydney, NSW 2000 Phone: 1300 722 206
International Pelvic Pain Society http://pelvicpain.org/docs/patients/Patient-Education-Brochure.aspx
Check out this information on available procedures for PND in Australia
Interstitial Cystitis IC Bladder Pain Syndrome
What is IC ? The following information is reproduced from the Melbourne bladder clinic website. A great link for a more in depth understanding of this difficult condition
BPS/IC is a chronic, debilitating disease of the bladder that is characterised an unpleasant bladder sensation, of more than 6 weeks’ duration and in the absence of infection or other identifiable causes.
How common is it ?
The incidence of BPS/IC is estimated at 8 to 1600 per 100 000. It affects men and women of all ages, cultures and socioeconomic backgrounds. It is more common in women and the male-to-female ratio is estimated to be about 1:10.
What are the causes ?
Despite extensive research, the exact causes of BPS/IC are still unclear.
What are the symptoms ?
Patients complain of frequent urination, sensation of constant urge to void and bladder pain. Chronic pain is an essential component of the syndrome and is described as worsening with bladder filling and is relieved by voiding. This pain is not only localised to the bladder, but can be felt throughout the pelvis (vagina, rectum, urethra, vulva).
How is it diagnosed ?
IC is a diagnosis of exclusion; meaning that other causes of these symptoms such as infection, overactive bladder (OAB), cancer, radiation or other forms of cystitis must be ruled out first.
Assessment should include a careful history, physical examination and investigations. In the history, BPS/IC patients void to avoid or relieve pain, whereas OAB patients void to avoid incontinence. The number of voids per day, sensation of urge to void and characteristics (location, severity, character) of the pain should be documented. A bladder diary may be useful here.
A urine test is done to exclude a urinary tract infection. It can also be done to look for cancer cells, especially in those with increased risks (over 50 years old, smoking history).
Cystoscopy and Urodynamics are considered as an aid to diagnosis, and are not necessary in uncomplicated cases.
Cystoscopy
- A cystoscopy (inspection of the inside of the bladder with a tubelike camera) can be done to look for features of IC, such as bladder ulcers or small bleeding points seen after distension of the bladder with sterile fluid. These findings are helpful but not necessary when making a diagnosis of IC.
- During the cystoscopy, a bladder biopsy can also be done to look for inflammatory cells in parts of the bladder wall.
- This can also rule out other bladder pathology like a bladder tumour, stone, or a urethral diverticulum (small out-pouching in the tube that drains the bladder).
Urodynamics:
- Rule out other diagnoses like an overactive bladder (OAB) or a poorly compliant (stiff) bladder.
- Can look for bladder outlet obstruction from failure to relax the pelvic floor during voiding.
Treatments for IC
First of all, it must be clear that there are no curative treatments; the treatments are aimed at alleviating the symptoms such that a patient can continue to have a reasonable quality of life. The patient should be counselled with regards to reasonable expectations for treatment outcomes. Treatment strategies should proceed from conservative ones to more invasive therapies. Some patients may benefit from a combination of treatments. Acceptable symptom control may also require trials of multiple therapeutic options. This website http://www.ichelp.org/ichope#.VIdot0cxmrV offers a great deal of advice on managing the pain of IC.
Conservative approaches:
- Diet changes: avoid food that triggers symptoms (eg. spicy foods, alcohol, caffeine).
- Altering the concentration or volume of urine, wither by fluid restriction or additional hydration.
- Application of local heat or cold over the bladder, trigger points and areas of hypersensitivity
- Strategies to manage flare-ups.
- Pelvic floor muscle relaxation / avoid pelvic floor strengthening exercises.
- Bladder retraining with urge suppression.
- Manual physical therapy (trigger point release by physiotherapist).
Multimodal management:
- May involve medications, stress management or manual therapy.
- A pain specialist is usually involved.
- It is difficult to predict which pain medication is most effective; this may require a trial of different medications.
Oral medications:
- Tricyclics antidepressants
- Some examples are amitriptyline, imipramine.
- Side effects are fatigue, drowsiness, weight gain, dry mouth (a third of patients cannot tolerate this).
- Sodium pentosan polysulfate (Elmiron)
- Acts by repairing defects in the bladder mucosa.
- A 3 to 6 month course is needed to demonstrate an effect.
- At a dose of 100mg three times a day, it is well tolerated and has few side effects.
- Cimetidine
- Dose of 400mg twice a day.
- Potential interaction with other medications.
- Vitamin D
Anitibiotics have no role in the management of BPS/IC in the absence of a proven urinary tract infection.
Bladder instillation therapy
A catheter is first inserted and the medication is then infused into the bladder for a period of about 15 – 20 minutes (depending on the drug). Multiple therapies are usually required. This route of administration provides high drug concentrations in the bladder and avoids systemic side effects. Long term remission is achievable in some patients, but most will relapse eventually and need more treatments. Some examples of these medications are dimethyl sulfoxide (DMSO) and Clorpactin.
Surgical therapy:
- Cystoscopy with bladder distension and electrical cautery of bladder ulcers if present.
- Some patients get relief of symptoms from this procedure, but most of the time, the effects will wear off.
- Trial of sacral neuromodulation (bladder pacemaker)
- A temporary stimulator is first inserted during the trial period; a permanent implant is then inserted if the patient demonstrates positive response.
- Anti spasm bladder injection
- This is more commonly used in patients with an overactive bladder (OAB).
- Urinary diversion with or without surgical removal of the bladder
- The ureters (tubes draining the kidneys to the bladder) are reimplanted into a segment of bowel which is diverted to the abdominal skin surface as a stoma (opening). A bag is then placed over the stoma to catch the urine.
- This option is often the last resort and can sometimes be very effective.
- Patients must understand that pain relief is not guaranteed even if the bladder is removed.
This link gives a nice recap on some of the services that I can help you with.
Please, if you have pelvic pain, see your GP and let’s try and get to the cause of your problem. If I can help you deal with overactive pelvic floor muscles, then this may go a long way in reducing and controlling your problem. Remember you don’t need a referral to come and see me. If I think you need other referral/investigations I will discuss these with you.
I look forward to seeing you.